

For generations, women have been told that painful periods are simply part of being female. Curling up in bed with a hot water bottle, cancelling plans every month or relying on painkillers to get through the workday has long been dismissed as routine. But for millions of women living with endometriosis, that normalisation often comes at a devastating cost.
According to the World Health Organization, endometriosis affects around one in ten women and girls of reproductive age globally. Yet despite its prevalence, diagnosis is frequently delayed, sometimes by seven to 10 years. During that time, many women are told they have irritable bowel syndrome (IBS), polycystic ovary syndrome (PCOS), urinary infections or simply “low pain tolerance”. Others leave consultation rooms with the reassurance that their ultrasound is normal, only to continue living with debilitating pain.
For specialists, the biggest challenge isn’t that endometriosis is rare. It’s that the disease continues to hide behind cultural assumptions, limited awareness and gaps in clinical training.
When pain becomes ‘normal’
One of the biggest reasons for delayed diagnosis begins long before a woman enters a doctor’s clinic.
“Painful periods have been normalised for generations,” says Dr. Abhishek Mangeshikar, endometriosis surgeon and director of the Indian Centre for Endometriosis. “A girl tells her mother she cannot get out of bed because of pain, and she’s often told, ‘I went through the same thing.’ That normalisation becomes the first filter.”
The result is that many women wait years before seeking specialist care, believing severe menstrual pain is simply something they must learn to tolerate.
Dr. Sucheta Talele, consultant gynaecologist and obstetrician at Inamdar Multispeciality Hospital, Pune, says symptoms frequently begin during adolescence but are repeatedly managed with painkillers rather than investigated further.
In India, menstrual stigma adds another layer of complexity. Conversations around periods are still considered uncomfortable in many households, making it difficult for young women to describe symptoms such as painful bowel movements, pelvic pain or pain during intercourse—all classic signs of endometriosis.
More than just period pain
One reason endometriosis continues to evade diagnosis is that it rarely presents the same way in every patient. Its symptoms often overlap with digestive disorders such as IBS, urinary tract conditions, PCOS and, in some cases, even appendicitis. Women may complain of bloating, constipation, diarrhoea, urinary urgency or chronic pelvic pain before anyone connects the dots.

“The biggest clue is that the symptoms follow a cyclical pattern,” explains Dr. Radhika Sheth, fertility specialist at Luma Fertility. “Pain tends to worsen before or during menstruation. Severe period pain, pain during intercourse, painful bowel movements around periods, heavy bleeding and fertility issues should all raise suspicion.”
Dr. Mangeshikar agrees, adding that the menstrual cycle itself often provides the answer. “IBS doesn’t care what day of your menstrual cycle it is. Endometriosis does. Any bowel, bladder or pelvic symptom that reliably worsens with menstruation deserves further evaluation.”
Even imaging can be misleading. Routine pelvic ultrasounds may appear completely normal, particularly in cases of deep infiltrating endometriosis.
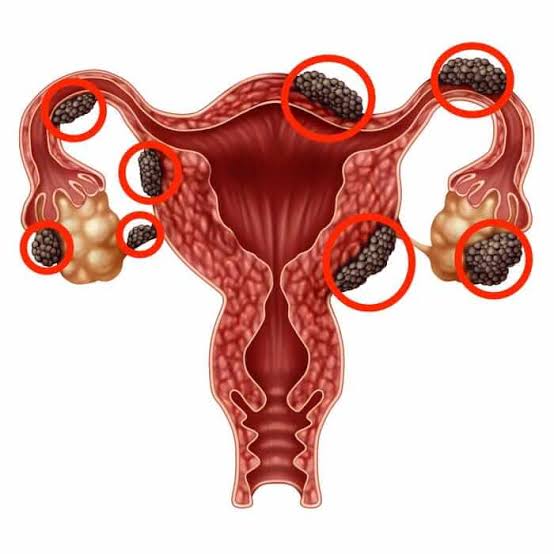
“A normal scan should never be used to rule out endometriosis,” says Dr. Mangeshikar. “It may only exclude ovarian cysts. Deep disease often sits behind the uterus, along nerves, on the bowel or bladder, where routine scans are not designed to look.”
Dr. Sucheta Talele echoes this concern, noting that because routine imaging may fail to detect early disease, diagnosis often depends on recognising clinical symptoms rather than relying solely on investigations.
The cost of waiting
Delayed diagnosis is not simply about living with pain for longer. It allows the disease to progress, often making treatment significantly more complex.
Dr. Shinjini Pande, consultant in gynaecology and laparoscopic surgery at P.D. Hinduja Hospital and Medical Research Centre, explains that chronic inflammation can gradually lead to dense scar tissue, distortion of pelvic anatomy and involvement of surrounding organs including the bowel and bladder. “As the disease progresses, surgery becomes far more extensive,” she says. “Instead of conservative treatment, patients may require complex procedures involving multiple organs.”
The impact on fertility is equally significant.
Endometriosis-related ovarian cysts can gradually reduce ovarian reserve, while inflammation and adhesions may interfere with fertilisation and implantation. Early diagnosis allows doctors to preserve fertility through timely medical or surgical intervention before irreversible damage occurs.
Less discussed, but equally important is the effect on the nervous system.
Persistent untreated pain can trigger a process known as central sensitisation, where the brain and spinal cord become increasingly sensitive to pain signals. “After years of untreated pain, the nervous system itself changes,” says Dr. Mangeshikar. “Pain becomes a disease of the nervous system, not just the endometriosis. That is one of the strongest arguments for diagnosing women earlier.”
The invisible burden
The physical symptoms are only part of the story. Years of being told that their pain is exaggerated or worse, psychological leave many women questioning their own experiences.
Dr. Pande notes that repeated dismissal by healthcare providers can lead to profound psychological distress, anxiety, depression and chronic fatigue. Sleep disruption, cognitive exhaustion and “brain fog” become common companions to chronic pain.
The condition also spills into every aspect of daily life. Missed workdays, repeated emergency visits and expensive treatments create financial strain. Pain during intercourse affects intimate relationships, while unpredictable flare-ups force many women to cancel plans, withdraw socially or reduce professional commitments. For many, the disease remains invisible to everyone except the person living with it.
Rethinking diagnosis
Experts believe shortening the diagnosis gap will require more than public awareness campaigns. Better education around menstrual health in schools, they argue, is a critical first step. Young girls and boys need to understand that pain severe enough to disrupt school, work or daily life is not a normal part of menstruation.
Doctors also point to the need for improved medical training. Endometriosis is often taught as a condition affecting the ovaries, despite its ability to involve multiple organs. “Primary care physicians need clearer referral pathways, and radiologists need specialised training to identify deep endometriosis through dedicated imaging protocols,” says Dr. Sheth.
Dr. Talele believes specialist referral systems and multidisciplinary care including gynaecologists, fertility experts, pain specialists, physiotherapists and psychologists can dramatically improve long-term outcomes.
Workplaces also have a role to play. Rather than treating menstrual pain as an occasional inconvenience, experts advocate flexible work policies that acknowledge chronic gynaecological conditions without forcing women to repeatedly justify their symptoms.
Changing the conversation
Perhaps the most significant shift, however, is cultural. For decades, women have been praised for silently enduring pain. Endometriosis challenges that narrative. “It is time we stop asking women to tolerate pain that prevents them from functioning,” says Dr. Pande. “Earlier diagnosis doesn’t just reduce symptoms, it protects fertility, mental wellbeing and quality of life.”
The conversation around women’s health has evolved considerably in recent years, with greater openness around menstruation, menopause and reproductive health. But experts say the next frontier is recognising that severe period pain is not something to simply live with.
Sometimes, the body is not asking for resilience.
It is asking to be believed.
Also Read:
From Stigma To Healing In Modern India
Booze Butt: When Your Gut Pushes Back on Alcohol
When Social Approval Decides What “Healthy” Looks Like





